irbesartan
 Generated by GPT-5-mini
Generated by GPT-5-miniExpansion Funnel Raw 84 → Dedup 0 → NER 0 → Enqueued 0
| irbesartan | |
|---|---|
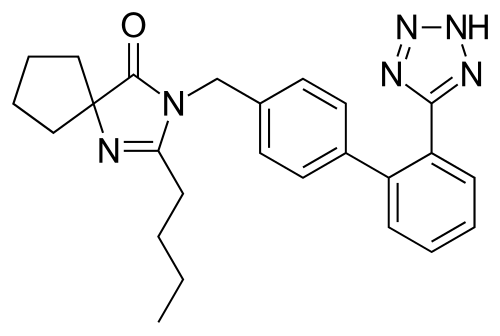 Fvasconcellos · Public domain · source | |
| Drug name | Irbesartan |
| Tradename | Avapro, Karvea, Aprovel, others |
| Routes of administration | Oral |
| Class | Angiotensin II receptor blocker |
| ATC | C09CA04 |
| Legal status | Rx-only (varies by country) |
irbesartan
Irbesartan is an angiotensin II receptor blocker used primarily to treat hypertension and nephropathy associated with type 2 diabetes. Developed for oral administration, it competes with other antihypertensive agents in clinical practice and guidelines endorsed by organizations such as the American Heart Association, European Society of Cardiology, and National Institute for Health and Care Excellence. The drug has been studied in randomized trials and large outcome studies, and it is marketed worldwide under multiple tradenames by multinational pharmaceutical companies.
Medical uses
Irbesartan is indicated for the management of essential hypertension in adults, often compared in trials with agents recommended by the National Heart, Lung, and Blood Institute, World Health Organization, American College of Cardiology, European Society of Hypertension, and Canadian Hypertension Education Program. It is also indicated for reducing progression of diabetic nephropathy in patients with type 2 diabetes and proteinuria, with evidence cited by American Diabetes Association, International Society of Nephrology, Kidney Disease: Improving Global Outcomes (KDIGO), and major nephrology centers such as Mayo Clinic, Cleveland Clinic, and Johns Hopkins Hospital. Clinical guidelines from NICE and national formularies like the British National Formulary include dosing regimens, and comparative effectiveness studies have evaluated irbesartan versus agents endorsed by European Medicines Agency and the U.S. Food and Drug Administration.
Irbesartan has been included in head-to-head trials against other antihypertensives listed by organizations such as American Society of Hypertension, Lancet, and New England Journal of Medicine investigators; collaborative research from institutions like Harvard Medical School, Stanford University School of Medicine, and University of Oxford informed prescribing patterns. It is used in combination with diuretics such as hydrochlorothiazide, with combination products approved in formularies managed by institutions including Veterans Health Administration and national health services like NHS England.
Contraindications and precautions
Use is contraindicated in pregnancy per advisories from American College of Obstetricians and Gynecologists, Royal College of Obstetricians and Gynaecologists, and WHO due to risks documented in teratology case series and drug safety communications from EMA and FDA. Concurrent use with aliskiren in patients with diabetes is discouraged by recommendations from European Society of Cardiology and regulatory safety warnings from Health Canada. Caution is advised in patients with renal artery stenosis, chronic kidney disease stages defined by KDIGO, and conditions described in guidance from European Renal Association and leading nephrology centers such as Mount Sinai Hospital and Hospital for Special Surgery.
Monitoring of serum potassium and renal function is recommended by consensus statements from American Society of Nephrology, European Renal Best Practice, and endocrine guidance from Endocrine Society when used with potassium-sparing drugs or mineralocorticoid receptor antagonists referenced in literature from British Cardiovascular Society.
Adverse effects
Common adverse reactions reported in clinical trials and pharmacovigilance databases maintained by FDA, EMA, and WHO Uppsala Monitoring Centre include dizziness, fatigue, and gastrointestinal complaints summarized in drug monographs from Drugs.com and compendia used by Merck Manual. Rare but serious events such as angioedema, hyperkalemia, acute kidney injury, and hypotension have been reported in case series published by centers including Mayo Clinic Clinics and in alerts from Health Canada and TGA (Therapeutic Goods Administration). Post-marketing surveillance reported adverse events to national pharmacovigilance programs coordinated with the Pharmacovigilance Risk Assessment Committee (PRAC) of the EMA.
Drug interaction profiles documented in tertiary sources used by Cleveland Clinic and Johns Hopkins highlight potential interactions with potassium supplements, nonsteroidal anti-inflammatory drugs referenced in guidelines from American College of Rheumatology, and concomitant renin–angiotensin system agents discussed in position papers by European Society of Cardiology.
Pharmacology
Irbesartan selectively antagonizes the angiotensin II type 1 (AT1) receptor, a mechanism characterized in basic research from laboratories at University of California, San Francisco, Salk Institute, and Max Planck Institute. Its antihypertensive effect is mediated by blockade of angiotensin II–induced vasoconstriction and aldosterone release, pathways detailed in foundational studies appearing in Nature, Science, and Journal of Clinical Investigation. Pharmacodynamic endpoints such as reduction in systemic vascular resistance and modulation of aldosterone were investigated in trials reported by investigators affiliated with Brigham and Women's Hospital, Beth Israel Deaconess Medical Center, and academic networks including ClinicalTrials.gov-registered studies.
Irbesartan’s receptor-binding profile and selectivity were elucidated using methods described in biochemical research from University of Cambridge, Imperial College London, and Massachusetts Institute of Technology.
Pharmacokinetics
Oral irbesartan has good bioavailability with peak plasma concentrations occurring within hours after dosing, parameters measured in pharmacokinetic studies from FDA submissions and independent research at institutions like University of Groningen and Università di Milano. It is metabolized primarily by hepatic pathways, with metabolites characterized in analytical reports submitted to EMA and published by research groups at Karolinska Institutet and Universidad Autónoma de Madrid. Elimination and half-life supporting once-daily dosing were reported in multicenter studies involving clinical pharmacology units at University College London and University of Toronto.
Population pharmacokinetic modeling and dose-adjustment guidance for renal impairment appear in reviews from Pharmacoepidemiology groups and regulatory labeling harmonized by agencies including FDA and EMA.
Chemistry and formulations
Irbesartan is a nonpeptide, biphenyl-tetrazole derivative; its chemical synthesis and structural characterization were reported in medicinal chemistry publications from research teams at Merck Research Laboratories and academic collaborators at University of Illinois Urbana–Champaign and ETH Zurich. Formulations include immediate-release tablets and fixed-dose combinations with hydrochlorothiazide, marketed by companies such as Bristol-Myers Squibb, Sanofi, and local generic manufacturers regulated by national agencies like Food and Drug Administration and European Commission directives on medicinal products.
Solid-state properties, stability data, and polymorph screening were investigated in pharmaceutical chemistry studies at University of Barcelona and Purdue University.
History and society
Development programs for irbesartan were led by industry teams and academic partners during the 1990s, with regulatory approvals by FDA and EMA in the late 1990s and early 2000s following clinical trials published in journals such as Lancet and New England Journal of Medicine. Patent, licensing, and market dynamics involved multinational corporations including Merck, Bristol-Myers Squibb, and generic manufacturers active within frameworks set by World Trade Organization agreements and national patent offices such as the United States Patent and Trademark Office and European Patent Office.
Societal impacts include inclusion on treatment formularies of major systems like NHS England, uptake in primary care influenced by recommendations from American Heart Association, and coverage decisions by payers including Centers for Medicare & Medicaid Services. Pharmacoeconomic analyses from research centers such as London School of Economics, Johns Hopkins Bloomberg School of Public Health, and Yale School of Medicine examined cost-effectiveness compared with other antihypertensive classes. Public health advisories and label changes were coordinated by regulatory bodies including FDA, EMA, and national ministries of health such as Health Canada and Australian Department of Health.
Category:Angiotensin receptor blockers