coronary artery disease
 Generated by GPT-5-mini
Generated by GPT-5-miniExpansion Funnel Raw 19 → Dedup 0 → NER 0 → Enqueued 0
| coronary artery disease | |
|---|---|
 | |
| Name | Coronary artery disease |
| Field | Cardiology |
| Symptoms | Chest pain, shortness of breath, fatigue |
| Complications | Myocardial infarction, heart failure, arrhythmia |
| Onset | Middle age to elderly |
| Causes | Atherosclerosis, thrombosis |
| Risks | Smoking, hypertension, diabetes, dyslipidemia |
| Diagnosis | ECG, coronary angiography, cardiac biomarkers, CT coronary angiography |
| Treatment | Lifestyle modification, pharmacotherapy, percutaneous coronary intervention, coronary artery bypass grafting |
coronary artery disease
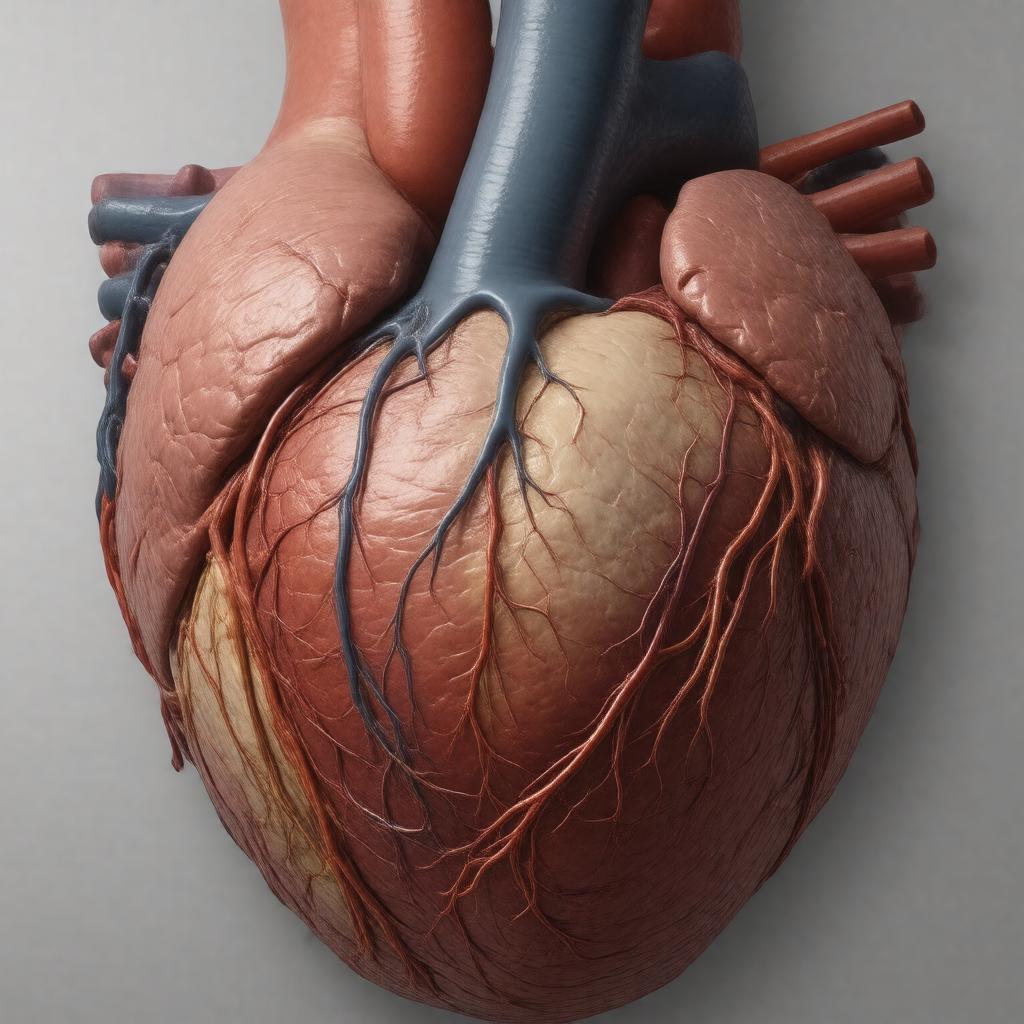
Coronary artery disease is a chronic cardiovascular condition characterized by narrowing of the coronary arteries that supply the heart, typically from atherosclerotic plaque buildup. It manifests across a spectrum from asymptomatic coronary atherosclerosis to stable angina and acute myocardial infarction, and it is a leading cause of morbidity and mortality worldwide. Clinical management integrates risk factor modification, diagnostics ranging from noninvasive imaging to invasive angiography, and reperfusion strategies performed by interventional cardiology teams.
Signs and symptoms
Patients often present with exertional chest discomfort or pressure (angina pectoris) described as substernal pain that may radiate to the neck, jaw, shoulder, or arm; associated features include diaphoresis, nausea, dyspnea, and syncope. Acute presentations include sudden severe chest pain consistent with ST-elevation myocardial infarction managed emergently by catheterization laboratories and cardiothoracic surgery teams. Many individuals, particularly older adults, women, and people with diabetes mellitus, may have atypical or silent ischemia detected incidentally on stress testing or imaging interpreted by specialists affiliated with tertiary centers such as Mayo Clinic, Cleveland Clinic, and major university hospitals. Chronic ischemic heart disease can lead to progressive exercise intolerance, heart failure symptoms evaluated by heart failure clinics, and arrhythmias managed by electrophysiology services.
Causes and risk factors
The principal etiologic process is atherosclerosis of coronary arteries influenced by modifiable and nonmodifiable risk factors. Modifiable factors include tobacco use linked to public health campaigns and regulations, hypertension managed according to guidelines from organizations like the American Heart Association and the European Society of Cardiology, dyslipidemia treated with statins following trials led by investigators at institutions such as Johns Hopkins Hospital and Massachusetts General Hospital, diabetes mellitus associated with endocrinology centers including Joslin Diabetes Center, obesity, physical inactivity, and unhealthy diets influenced by food policies and industry practices. Nonmodifiable factors include advancing age, male sex, and family history, with genetic predispositions studied at research centers like Broad Institute and Wellcome Sanger Institute. Socioeconomic determinants and disparities examined by public health agencies such as the World Health Organization and national institutes contribute to population risk.
Pathophysiology
Atherosclerotic plaque formation begins with endothelial injury and lipid retention within the intima, progressing through inflammatory cell infiltration, foam cell formation, fibrous cap development, and potential plaque rupture with superimposed thrombosis. Platelet activation and coagulation cascade engagement can produce occlusive thrombi causing myocardial necrosis characterized in classic descriptions by pathologists and clinicians from institutions like St. Bartholomew's Hospital and academic departments worldwide. Ischemia leads to metabolic shifts in cardiomyocytes, release of cardiac biomarkers first characterized in cohorts followed at centers such as Framingham Heart Study and detectable by assays developed in clinical laboratories. Collateral vessel development and ischemic preconditioning are adaptive processes studied in basic science labs at universities including Harvard University and Oxford University.
Diagnosis
Diagnostic evaluation integrates history and physical examination with electrocardiography, cardiac biomarkers (troponin), stress testing modalities, and imaging. Resting ECGs and serial biomarkers are frontline tools in emergency departments affiliated with major health systems for acute coronary syndromes. Noninvasive imaging options include exercise ECG interpreted by sports medicine programs, stress echocardiography performed in cardiology clinics, nuclear myocardial perfusion imaging using radiotracers developed in radiopharmaceutical research centers, and CT coronary angiography offered at tertiary imaging centers. Invasive coronary angiography in catheterization laboratories remains the gold standard to define coronary anatomy and guide revascularization performed by interventional cardiologists credentialed by societies like the Society for Cardiovascular Angiography and Interventions. Fractional flow reserve and intravascular ultrasound are adjuncts used in specialized centers.
Prevention and screening
Primary prevention emphasizes smoking cessation programs supported by public health initiatives, blood pressure control per guideline committees, lipid-lowering therapy with statins and PCSK9 inhibitors evaluated in randomized trials from pharmaceutical research groups, glycemic control for diabetes managed by endocrinology societies, weight management, and promotion of physical activity through community health campaigns. Secondary prevention after an acute event includes antiplatelet therapy, beta blockers, ACE inhibitors or ARBs, and cardiac rehabilitation programs often housed in hospital-based services. Screening strategies using risk calculators derived from cohort studies such as the Framingham Heart Study and pooled international cohorts inform statin eligibility and imaging decisions; population screening remains debated by panels convened by agencies like the U.S. Preventive Services Task Force.
Treatment
Treatment spans lifestyle modification, pharmacotherapy, and revascularization. Medical therapy includes antiplatelet agents such as aspirin and P2Y12 inhibitors tested in multicenter trials, high-intensity statins, antihypertensives, and antianginal drugs like nitrates and beta blockers managed by cardiology teams. Percutaneous coronary intervention with stent placement is performed in catheterization laboratories using drug-eluting stents produced by device manufacturers and evaluated in trials coordinated by cooperative groups. Coronary artery bypass grafting is performed by cardiothoracic surgeons in centers such as Cleveland Clinic and Mount Sinai Hospital for multivessel disease or left main coronary stenosis, with graft conduits including internal mammary artery and saphenous vein. Acute ST-elevation myocardial infarction requires timely reperfusion via primary PCI or thrombolysis when PCI is unavailable, protocols developed by emergency medicine and cardiology consortia.
Epidemiology and outcomes
Coronary artery disease is a leading cause of death globally with incidence and prevalence varying by region, socioeconomic status, and risk factor burden tracked by organizations such as the World Health Organization, Centers for Disease Control and Prevention, and national health ministries. Longitudinal cohort studies like the Framingham Heart Study and international consortia provide data on trends in mortality and recurrent events; declines in age-adjusted death rates in high-income countries have been attributed to risk factor control and advances in acute care, while low- and middle-income countries face rising burdens. Outcomes depend on timeliness of reperfusion, access to secondary prevention, and comorbidities, with ongoing research from academic institutions and trial networks aimed at reducing residual risk.
Category:Cardiovascular diseases