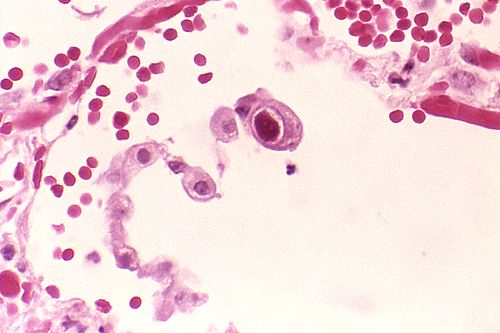
Cytomegalovirus
This article was accepted into the corpus but its outbound wikilinks were never NER-processed — typical at the deepest BFS hop or when the run's entity cap was reached. No expansion funnel to show.
| Cytomegalovirus | |
|---|---|
 Public domain · source | |
| Name | Cytomegalovirus |
| Virus group | dsDNA virus |
| Family | Herpesviridae |
| Subfamily | Betaherpesvirinae |
| Genus | Cytomegalovirus (genus) |
| Species | Human cytomegalovirus |
Cytomegalovirus is a ubiquitous human herpesvirus with a large double‑stranded DNA genome that establishes lifelong latency after primary infection. It is a major cause of congenital infection and opportunistic disease in immunocompromised persons, and it has been studied in contexts ranging from transplant medicine to perinatal care. Research into its molecular biology, epidemiology, and immune interactions links work across virology laboratories, public health agencies, and clinical centers worldwide.
Virology
Human cytomegalovirus is a member of the Herpesviridae family and the Betaherpesvirinae subfamily, characterized by enveloped virions and a linear dsDNA genome of approximately 235 kilobase pairs. The virion architecture includes a capsid, tegument, and lipid envelope containing glycoproteins such as gB and gH/gL complexes; structural and functional studies have been performed at institutions like the Max Planck Institute and the Wadsworth Center. The genome encodes more than 200 predicted open reading frames and numerous noncoding RNAs, with annotation efforts contributed by teams at the Broad Institute and the Wellcome Trust Sanger Institute. Viral entry engages cellular receptors, with research implicating heparan sulfate proteoglycans and integrins; key mechanistic insights have been reported by groups at the University of Cambridge and the University of California, San Francisco. CMV demonstrates cell‑type tropism for fibroblasts, epithelial cells, endothelial cells, monocytes, and macrophages; tropism studies have been pursued at the Rockefeller University and the Pasteur Institute. Viral replication occurs in nuclear replication compartments, and virion assembly and egress involve the trans‑Golgi network; mechanistic models were developed in laboratories at the Johns Hopkins University and the University of Pennsylvania.
Epidemiology
Seroprevalence varies by region, socioeconomic status, and age, with higher rates reported in parts of Africa, Asia, and Latin America and lower rates in Northern Europe and parts of North America; large population surveys have been conducted by the Centers for Disease Control and Prevention and the European Centre for Disease Prevention and Control. Transmission routes include body fluids such as saliva, urine, breast milk, sexual contact, blood transfusion, organ transplantation, and vertical congenital transmission; surveillance programs at the World Health Organization and transplant registries at the American Society of Transplantation track outcomes. Outbreak investigations in neonatal nurseries and pediatric day care centers have been reported by public health departments in cities such as London, New York City, and Toronto. Risk factors for primary infection and reinfection include exposure in households, workplaces like daycare centers, and regions with limited access to maternal health services; demographic analyses have been performed by teams at the University of Oxford and Harvard University.
Clinical Manifestations
Most primary infections in immunocompetent adults are asymptomatic or produce a mononucleosis‑like syndrome; clinical descriptions appear in reports from hospitals including Massachusetts General Hospital and Guy's and St Thomas' NHS Foundation Trust. Congenital infection can lead to sensorineural hearing loss, neurodevelopmental delay, and intracranial calcifications; pediatric case series have been published by the Children's Hospital of Philadelphia and the Great Ormond Street Hospital. In immunocompromised patients, including solid‑organ and hematopoietic stem cell transplant recipients and persons with advanced HIV/AIDS, CMV causes end‑organ disease such as retinitis, colitis, pneumonitis, and encephalitis; outcomes data derive from registries at the European Society for Blood and Marrow Transplantation and the American Academy of HIV Medicine. Congenital CMV remains a leading nonhereditary cause of childhood sensorineural hearing impairment, documented in studies from the Centers for Disease Control and Prevention and pediatric cohorts at the Karolinska Institutet.
Diagnosis
Laboratory diagnosis employs viral culture, antigenemia assays, nucleic acid amplification testing (PCR), and serology (IgM, IgG, avidity testing). Quantitative PCR viral load monitoring is standard in transplant centers such as those at Mayo Clinic and the University of California, Los Angeles to guide preemptive therapy. For congenital infection, testing of newborn saliva or urine within the first three weeks of life is recommended by perinatal units at institutions like Johns Hopkins Medicine and Mount Sinai Hospital. Histopathology demonstrating characteristic cytomegalic cells with intranuclear inclusions has been described in case series from the Royal Free Hospital and the Hospital for Sick Children (Toronto). Novel diagnostic modalities, including digital PCR and next‑generation sequencing, are under evaluation in consortia involving the National Institutes of Health and the Wellcome Trust.
Treatment and Prevention
Antiviral therapy includes nucleoside analogues such as ganciclovir, valganciclovir, foscarnet, and cidofovir; clinical trials and guideline recommendations are available from the Infectious Diseases Society of America and transplant centers at Stanford University Medical Center. Drug resistance mediated by UL97 and UL54 mutations is managed by susceptibility testing and alternative regimens; resistance surveillance has been reported by laboratories at the Veterans Affairs Medical Centers and academic centers like Yale School of Medicine. Prevention strategies encompass screening of blood products by transfusion services at the American Red Cross and donor screening in transplantation coordinated by the United Network for Organ Sharing. Vaccine development efforts have involved platforms tested in trials sponsored by institutions including the National Institute of Allergy and Infectious Diseases and companies collaborating with the Bill & Melinda Gates Foundation; maternal immunization and passive immunoprophylaxis remain active research priorities.
Pathogenesis and Immune Response
CMV pathogenesis reflects viral latency in myeloid progenitors and reactivation driven by immunosuppression or inflammation; foundational studies originated at the Salk Institute and the Fred Hutchinson Cancer Center. The immune response involves innate sensors, NK cells, and robust CMV‑specific CD4+ and CD8+ T cell responses; T cell immunology has been characterized by investigators at the La Jolla Institute for Immunology and the Pasteur Institute. Viral immune evasion includes modulation of MHC class I and II antigen presentation, cytokine mimicry, and interference with NK cell ligands; molecular mechanisms were elucidated in research programs at the University of Toronto and the Max Delbrück Center for Molecular Medicine. Understanding the balance between latency, reactivation, and immune control informs transplantation protocols at centers such as Cleveland Clinic and guides vaccine strategies pursued by the Bill & Melinda Gates Foundation and academic consortia.
Category:Herpesviruses